Article Text

Abstract
This report describes a case of pulmonary epithelioid haemangioendothelioma in which the tumour cells expressed the glucocorticoid receptor and 11β-hydroxysteroid dehydrogenase. The patient, a 15 year old girl, who had no other complaints or past illnesses, was found to have an abnormal shadow on a chest roentgenogram obtained at a school medical examination. Multiple nodular shadows in the bilateral lungs were also confirmed by computerised axial tomography scan. A diagnosis of pulmonary epithelioid haemangioendothelioma was made on the basis of lung biopsy specimens. The tumour cells were immunohistochemically positive for factor VIII related antigen, CD31, and CD34, but not surfactant apoprotein A. In addition, almost all of the tumour cells showed simultaneous expression of the glucocorticoid receptor and 11β hydroxysteroid dehydrogenase, suggesting that steroid treatment would be effective.
- HSD, hydroxysteroid dehydrogenase
- PAS, periodic acid Schiff
- PEH, pulmonary epithelioid haemangioendothelioma
Statistics from Altmetric.com
- HSD, hydroxysteroid dehydrogenase
- PAS, periodic acid Schiff
- PEH, pulmonary epithelioid haemangioendothelioma
Pulmonary epithelioid haemangioendothelioma (PEH) is a rare vascular tumour characterised by epithelioid-like endothelial cells.1,2 This tumour also arises at other sites, typically soft tissue, bone, or liver. To date, approximately 50 cases of PEH have been recorded in the English literature, with a female : male patient ratio of 4 : 1. Classically, it presents as asymptomatic bilateral pulmonary multiple nodules in young women. It is generally considered to be a low grade malignant tumour with unpredictable behaviour, resulting in relatively short average patient survival,3,4 although cases showing sporadic partial spontaneous regression have been reported.5 We present a case of PEH expressing the glucocorticoid receptor and 11β hydroxysteroid dehydrogenase (HSD).
CASE REPORT
A 15 year old girl was incidentally found to have abnormal shadows in the bilateral lungs on a chest roentgenogram obtained at a school medical examination, and was admitted to Yamagata Prefectural Nihonkai Hospital. She had no significant complaints, past illnesses, or familial history.
Routine laboratory data were within normal limits except for an increased concentration of C reactive protein (4 mg/litre). Plain chest roentgenography disclosed multiple sharply demarcated nodular densities throughout both lungs, without evidence of mediastinal lymphadenopathy. A computerised axial tomography scan of the bilateral lungs revealed multiple nodules up to 3 mm in diameter (fig 1).

Enhanced computerised axial tomography of the left lung. Note the multiple small nodules.
Biopsy specimens were obtained from greyish miliary sized lesions, which were seen to protrude slightly from the lung surface by video assisted thoracoscopy. The tumour was diagnosed as PEH. Up to the time of writing, no tumour metastases to other sites have been detected.
METHODS
After thorough fixation in 10% formalin, the biopsy specimens were embedded in paraffin wax. Sections were cut, then stained with haematoxylin and eosin. Special stains included periodic acid Schiff (PAS), alcian blue, Masson's trichrome, and silver impregnation.
Immunohistochemical staining of 4 μm thick sections was performed using the labelled streptavidin–biotin–peroxidase complex method. Table 1 lists the antibodies used. For antigen retrieval, dewaxed sections were treated in a microwave oven in 0.01M ethylenediamine tetra-acetic acid (pH 8.0) (Wako Pure Chemicals, Tokyo, Japan) for 23 minutes at 90°C (400 W). Positive reactions were visualised with 3,3`-diaminobenzidine (Muto Pure Chemicals, Tokyo, Japan) with haematoxylin counterstaining. Negative controls were run in parallel by replacing the specific antibody with 0.01M phosphate buffered saline (pH 7.4) or mouse IgG (Dako, Glostrup, Denmark).
Results of immunohistochemistry
The following tissues were used as positive controls: three cases of lung adenocarcinoma (bronchioloalveolar type) for factor VIII related antigen, CD31, CD68, epithelial membrane antigen, and surfactant apoprotein A; two cases of malignant melanoma for HMB-45; two cases of gastrointestinal stromal tumour for CD34 and c-kit (CD117); three cases of breast cancer (papillotubular carcinoma) for oestrogen and progesterone receptors; two cases of chronic tonsillitis for cell cycle markers (proliferating cell nuclear antigen, cyclin A, cyclin B1, and cyclin D1); liver and kidney tissues from two postmortem cases for 11β HSD type 1 and type 2, respectively; and bone marrow tissues from two cases of chronic lymphocytic leukaemia for the glucocorticoid receptor.
When evaluating immunoreactivity for cell cycle markers (proliferating cell nuclear antigen, cyclin A, cyclin B1, and cyclin D1) and the glucocorticoid receptor both positive cells and total cells in tumour nodules were counted at high power (×400), and at least 30 microscopic fields were observed for each immunostain. Immunoreactivity was indicated as mean value (SD) of percentage ((positive cells/total cells) × 100).
PATHOLOGICAL FINDINGS
Histologically, the non-encapsulated nodules consisted of polygonal to plump cells, characterised by deeply indented nuclei with finely granular chromatin and occasional nucleoli, and abundant and frequently vacuolated cytoplasm (fig 2A,B). They often lay singly or formed microscopic nests or short narrow vascular slits, separated by abundant fibromyxoid or hyalinised stroma, which was also demonstrated by silver impregnation (fig 2C). Viable tumour cells were embedded in a stroma that was stained intensely with PAS and alcian blue.
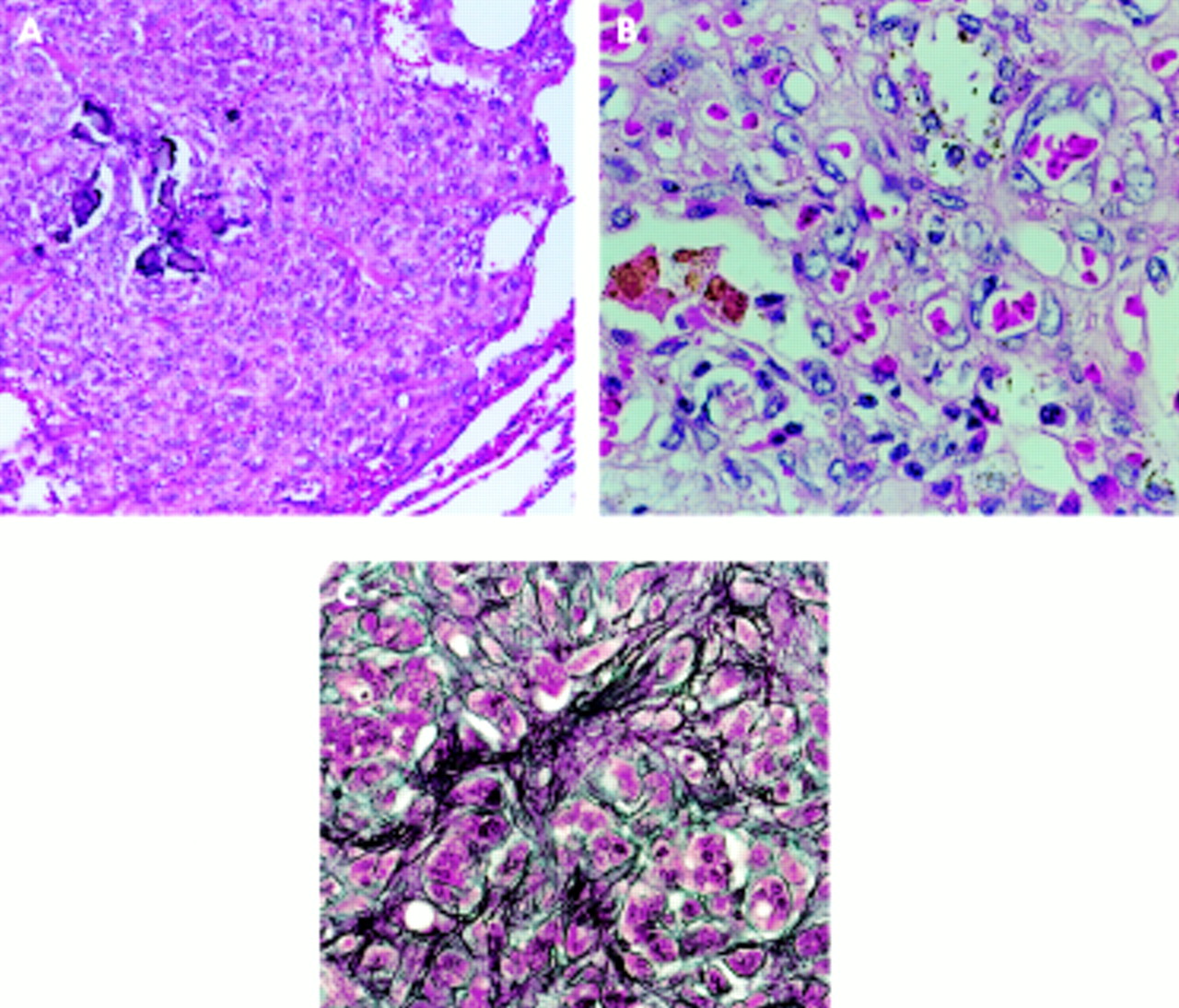
Histology of the tumour. (A) Low power view of a tumour nodule with calcification. Haematoxylin and eosin stain; original magnification, ×133. (B) High power view of a tumour nodule exhibiting several intracytoplasmic lumina containing red blood cells. Haematoxylin and eosin stain; original magnification, ×540. (C) Individual tumour cells or small groups of them are surrounded by reticulin fibres. Silver impregnation; original magnification, ×260.
Immunohistochemically, most of the tumour cells were positive for factor VIII related antigen, CD31 (fig 3A) and CD34 (table 1). They also expressed the glucocorticoid receptor (fig 3B) and 11β HSD type 1 (fig 3C) and type 2 (fig 3D). Most cells were positive for proliferating cell nuclear antigen. In contrast, the average labelling index of cyclin A, which is expressed on cells in the S–G2–M phase of the cell cycle, was 2.8%; that of cyclin B1, which is expressed on cells in G2–M phase, was only 0.55%; and that of cyclin D1, which is expressed on cells in G1 phase, was 25.53%.

{kind=link}
{kind=link}
{kind=link}
Immunostaining of (A) CD31, (B) glucocorticoid receptor, (C) 11β hydoxysteroid dehydrogenase type 1, and (D) 11β hydoxysteroid dehydrogenase type 2. Most of the tumour cells are positive. Original magnification, ×260.
DISCUSSION
Apparently benign lesions of haemangioendothelioma are best treated by wide local excision and apparently malignant ones by radical excision. Various chemotherapeutic regimens including steroid, isoniazid, and azathioprine have been tried, but have not proved helpful.6 Oestrogen and progesterone receptors are not exclusively detected in PEH in the lung.7 Patient mortality is higher for lung and liver lesions (65% and 35%, respectively), which have a greater tendency to be multifocal, compared with 13% for soft tissue lesions. The average survival of patients with lung lesions is 6.4 years.3,6
Cyclin A and cyclin B1 recognise cells in the S–G2–M phase and G2–M phase of the cell cycle, respectively, and their expression is correlated with a higher cell proliferation rate. Overexpression of cyclin A rather than proliferating cell nuclear antigen is related to poor differentiation and poor prognosis of colon cancer.8 In our case, the mean (SD) labelling indices of cyclin A, cyclin B1, and cyclin D1 were 2.80% (0.30%), 0.50% (0.32%), and 25.53% (2.47%), respectively, indicating that this tumour was slow growing although cells in G1 phase labelled with cyclin D1 were frequently observed; this was also reflected in the low mitotic activity of the tumour cells.
In this case of PEH, we were able to demonstrate the expression of the glucocorticoid receptor and 11β HSD types 1 and 2. 11β HSD is one of the most important enzymes in glucocorticosteroid metabolism.9 11β HSD type 1 in the liver acts mainly as an oxidoreductase to maintain circulating concentrations of glucocorticoid. In contrast, 11β HSD type 2 inactivates glucocorticosteroids and plays a pivotal role in the distal tubule, where it protects the mineralocorticoid receptor from occupation, thus endowing specificity on a non-selective receptor.9 In mineralocorticoid target tissues, 11β HSD type 2 converts cortisol to cortisone. The previous ineffectiveness of steroid treatment for PEH may have resulted from the presence of a glucocorticoid inhibitory enzyme. Recently, inhibition of 11β HSD type 2 activity with the liquorice compound glycyrrhetinic acid in breast cancer cell lines in vitro has been shown to enhance the antiproliferative effect of glucocorticoids.10 Taken together, the present findings emphasise that in our patient with PEH, who simultaneously expressed both the glucocorticoid receptor and 11β HSD types 1 and 2, glucocorticoid administration with an inhibitor of 11β-HSD type 2, such as glycyrrhetinic acid, may be therapeutically useful. In the future, follow up with a larger series is needed.