Article Text

Abstract
Background: Cell adhesion molecules and endothelial growth factors have an important role in the infiltrating of rheumatoid synovium with mononuclear cells, leading to the initiation and progression of the disease.
Objective: To investigate whether the serum profile of soluble adhesion molecules and of vascular endothelial growth factor (VEGF) is associated with the histological appearance of rheumatoid arthritis (RA).
Methods: Serum levels of soluble intercellular adhesion molecule-1 (sICAM-1), vascular cell adhesion molecule-1 (sVCAM-1), E-selectin (sE-selectin), and VEGF were assessed by enzyme linked immunosorbent assay (ELISA) in 40 patients with RA and 32 patients with osteoarthritis (OA).
Results: Histological analysis of synovium specimens distinguished two types of rheumatoid synovitis. Twenty four RA samples presented diffuse infiltrates of mononuclear cells without any further microanatomical organisation, whereas in the remaining 16 samples lymphocytic follicles with germinal centre-like structures were identified. In comparison with patients with OA, constituting a control group, higher serum concentrations of sICAM-1 (p<0.001), sVCAM-1 (p<0.001), sE-selectin (p<0.01), and VEGF (p<0.001) were detected in patients with RA. Raised concentrations of sICAM-1, sVCAM-1, and VEGF dominated in the serum of patients with RA with follicular synovitis compared with those with diffuse synovitis (p<0.01 for all comparisons). The serum concentrations of sICAM-1, sVCAM-1, and VEGF correlated with markers of disease activity such as the erythrocyte sedimentation rate and C reactive protein levels. Furthermore, the clinical data analysed in our study indicated that patients with RA with follicular synovitis tend to have more severe disease.
Conclusions: The distinct histological appearances of rheumatoid synovitis associated with different serum profiles of sICAM-1, sVCAM-1, and VEGF reflect varied clinical activity of the disease and confirm RA heterogeneity. Patients with different histological forms of synovitis may respond differently to the treatment regimens.
- sICAM-1
- sVCAM-1
- sE-selectin
- VEGF
- rheumatoid arthritis
- histology
- CRP, C reactive protein
- DMARDs, disease modifying antirheumatic drugs
- ELISA, enzyme linked immunosorbent assay
- ESR, erythrocyte sedimentation rate
- OA, osteoarthritis
- RA, rheumatoid arthritis
- sCAM, soluble cellular adhesion molecule
- sE-selectin, soluble E-selectin
- sICAM-1, soluble intercellular adhesion molecule-1
- sVCAM-1, soluble vascular cell adhesion molecule-1
- VEGF, vascular endothelial growth factor
Statistics from Altmetric.com
- CRP, C reactive protein
- DMARDs, disease modifying antirheumatic drugs
- ELISA, enzyme linked immunosorbent assay
- ESR, erythrocyte sedimentation rate
- OA, osteoarthritis
- RA, rheumatoid arthritis
- sCAM, soluble cellular adhesion molecule
- sE-selectin, soluble E-selectin
- sICAM-1, soluble intercellular adhesion molecule-1
- sVCAM-1, soluble vascular cell adhesion molecule-1
- VEGF, vascular endothelial growth factor
A prominent feature of rheumatoid synovitis is the accumulation of lymphocytes, macrophages, and fibroblasts involved in the synovial tissue destruction processes. Increased angiogenesis and the proliferation of the synovium lining layer may be also noticed.1–3 In some of the rheumatoid synovial specimens, lymphoid follicles were found.4–6 These T-B cell aggregates, which sometimes form germinal-like centres, seem to have an important role in the pathogenesis of rheumatoid arthritis (RA).7,8 Therefore, in addition to genetic, biological, and clinical heterogeneity, histological heterogeneity of RA has also been suggested.5,9–12
The existence of at least three different histological types of rheumatoid synovitis has been demonstrated.6 Most rheumatoid synovia displayed only a diffuse infiltrate of mononuclear cells, without any further microanatomical organisation. Lymphocytic follicles were found only in about one third of RA specimens. Some of them are germinal centre-like structures with a central accumulation of B cells surrounded by T cells. Only individual patients with RA displayed necrobiotic granulomas with a fibrinoid necrotic centre lined by a collar of histiocytes. The presence of follicular structures and granulomatous necrobiosis was not seen in samples from the same patient.6 It was suggested that patients with lymphoid follicles have a greater degree of immunological activation, and greater potential for tissue destruction.5,6,13,14 Moreover, each of the histological forms of rheumatoid synovitis was associated with a specific pattern of cytokine production in the synovium5,6 and of cytokines13 or matrix metalloproteinase14 levels in the serum of the patients with RA.
The destruction of synovial tissue in RA is mediated by cytokines and matrix metalloproteinases produced by macrophages and fibroblasts, and seems to be controlled by lymphocytes.15,16 Activation, circulation, and migration of mononuclear cells to inflammatory sites are regulated by adhesion molecules such as intercellular adhesion molecule-1 (ICAM-1), vascular cell adhesion molecule-1 (VCAM-1), or E-selectin.17–20 Inflammatory cell migration is also increased owing to the stimulation of synovial tissue neovascularisation by endothelial growth factors.21,22 Recently it was reported also that soluble forms of VCAM-1 (sVCAM-1) and of E-selectin (sE-selectin) might act as angiogenic mediators.23 Therefore, cell adhesion molecules (CAMs) and endothelial growth factors have an important role in the infiltration of rheumatoid synovium with mononuclear cells and seem to play a part in the initiation and progression of the disease. This study aimed at investigating whether the profile of soluble adhesion molecules and of vascular endothelial growth factor (VEGF) is associated with histopathological forms of the rheumatoid synovitis.
PATIENTS AND METHODS
Study groups
We studied 40 patients who fulfilled the American College of Rheumatology 1987 revised criteria for RA24 and 32 patients with osteoarthritis (OA), who comprised the control group. Synovial samples were obtained during hip or knee joint orthopaedic surgery from all patients with RA and OA who were entered into the study. Table 1 shows the characteristics of the patient groups.
Patient characteristics. Data presented as means (SD)
Clinical and laboratory analysis
The assessment included the number of tender joints (Ritchie's index),25 number of swollen joints, erythrocyte sedimentation rate (ESR), C reactive protein (CRP) concentration measured by a radial immunodiffusion kit (Nanorid, The Binding Site Ltd, Birmingham, UK), and the rheumatoid factor level. Radiological assessment of joint destruction was performed according to Steinbrocker's criteria.26
Histopathological evaluation
Synovial specimens underwent routine staining with haematoxylin and eosin. Histological analysis, which included assessment of the density and microanatomical organisation of the mononuclear cell infiltrate, was carried out as previously described.6,13,14
Serum specimens preparation
Blood samples were clotted for 30 minutes and then centrifuged for 10 minutes at 1000 g. Serum aliquots were frozen at –80°C immediately after collection.
Enzyme linked immunosorbent assay (ELISA)
The serum concentrations of sICAM-1, sVCAM-1, and sE-selectin were measured with commercial ELISA kits (Bender MedSystems, Vienna, Austria). Levels of VEGF were assessed by an ELISA kit from R&D Systems, Wiesbaden-Nordenstadt, Germany. Assays were carried out according to the manufacturer's instructions. The sensitivities were 3.3 ng/ml for sICAM-1, 0.9 ng/ml for sVCAM-1, 0.5 ng/ml for sE-selectin, and 9.0 pg/ml for VEGF.
Statistical analysis
The normally distributed data were analysed by unpaired Student's t test. The Mann-Whitney U test was used to evaluate the differences between non-normally distributed data such as the patient's age, disease duration, ESR, CRP, sICAM-1, sVCAM-1, and VEGF values. The probability of differences in frequency distributions was determined by a χ2 test. Data were correlated by Spearman's rank order test. p Values <0.05 were considered significant.
RESULTS
Histological patterns
RA synovia samples were characterised by mononuclear cell infiltrates of various densities. Infiltrates consisted mainly of lymphocyte-like and macrophage-like cells and were of perivascular and interstitial types. Twenty four specimens showed only diffuse infiltration of mononuclear cells, without any additional microanatomical organisation, and were classified as diffuse rheumatoid synovitis. Lymphocytes forming follicular conglomerates, sometimes with germinal centre-like structures, were found in 16 samples. These synovia were categorised as follicular synovitis. In rheumatoid synovia the formation of new vessels was also detected, which were especially dense around follicular structures. Other findings included synovial lining layer proliferation and rare giant-like cells. Formation of necrobiotic granulomas was not seen. OA synovial specimens demonstrated mild mononuclear cell infiltrates with rare capillary neoangiogenesis formation. Figure 1 presents typical examples of OA and two different forms of rheumatoid synovitis.

Histological pictures of RA and OA synovia. Representative samples are presented for the groups of patients analysed. (A) RA synovium specimen displaying diffuse mononuclear cell infiltrates without specific microanatomical organisation. (B) RA sample with lymphocytic follicular aggregates. (C) OA synovium with mild mononuclear cell infiltration. Original magnification ×100.
Demographic and clinical findings
No differences in sex profile, age, or disease duration between patients with both histological types of RA and with OA were seen. The ESR and CRP concentrations were higher in RA than in the OA group (in all cases p<0.001), especially in patients with follicular rheumatoid synovitis (table 1). Patients with the follicular type of RA were also characterised by a higher number of swollen joints than those with diffuse synovitis (p<0.01). Methotrexate treatment and radiologically more advanced joint destruction (stage III or IV according to Steinbrocker's criteria) occurred more often among patients with lymphocytic follicles than among those without (p<0.05 for both comparisons) (table 1). No other differences in clinical measures of the disease activity between histological types of RA were found.
Serum soluble cell adhesion molecule profiles
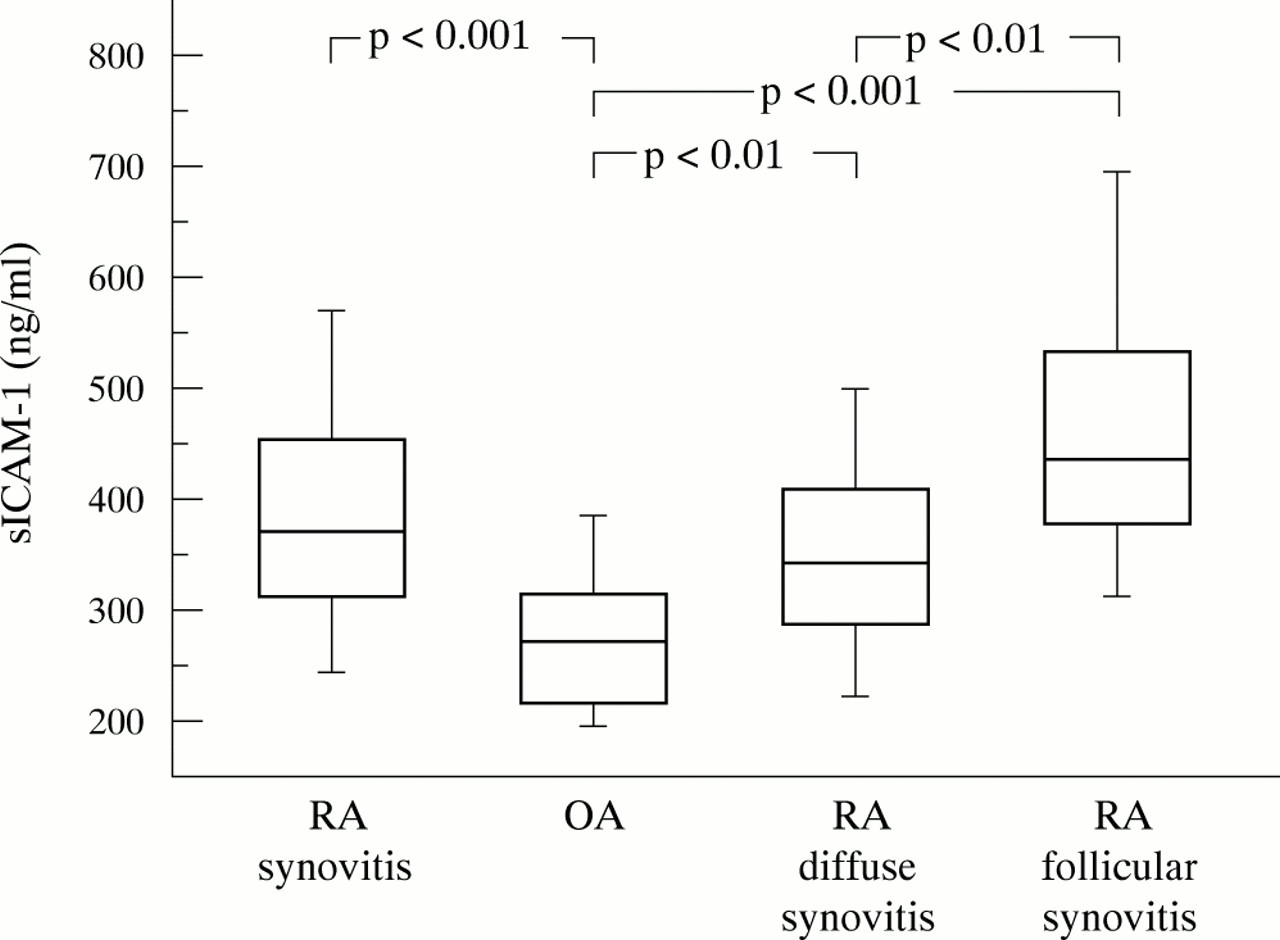
An ELISA technique was used to measure serum soluble adhesion molecules concentrations. Our main goal was to evaluate whether the serum soluble adhesion molecules and VEGF display distinct patterns in patients with different histopathological forms of rheumatoid synovitis. Figure 2 and table 2 show that the concentrations of sICAM-1 in serum were raised in all patients with RA, and among those with diffuse or follicular synovitis compared with patients with OA (p<0.001, p<0.01, and p<0.001 respectively). The concentration of sICAM-1 was especially high in patients with the follicular type of synovitis, distinguishing them from those with diffuse synovitis (p<0.01).
Serum concentrations of soluble adhesion molecules and vascular endothelial growth factor in patients with RA and OA. Data are presented as means (SD), median (25–75 centile). Figures 2–5 show the significances of the differences between patients groups

Serum concentrations of sICAM-1 in the patients studied. Assessment was based on an ELISA technique. The box plots represent median (line), 25th and 75th centiles (box), and 10th and 90th centiles (whiskers).
The concentrations of sVCAM-1 were also increased in all RA and in both histological forms of synovitis relative to patients with OA (p<0.001 for all comparisons) (fig 3 and table 2). sVCAM-1 dominated in follicular synovitis and could clearly differentiate this subgroup of patients with RA (p<0.01).

Serum concentrations of sVCAM-1. The measurement of sVCAM-1 was performed and shown as described in the legend to fig 2.
Serum soluble E-selectin (sE-selectin) levels were also raised in all patients with RA and with diffuse or follicular synovitis as compared with patients with OA (p<0.01, p<0.05, and p<0.01 respectively) (fig 4 and table 2). However, sE-selectin concentrations did not differ significantly between the two histopathological forms of RA.

Serum concentrations of sE-selectin were analysed and presented as described in the legend to fig 2.
Serum vascular endothelial growth factor concentrations
Serum VEGF dominated in all patients with RA and in both histological forms of rheumatoid synovitis, in comparison with patients with OA (p<0.001 for all comparisons) (fig 5 and table 2). The highest levels of VEGF were found among the patients with follicular type of RA and distinguished them from those with only diffuse infiltrates in rheumatoid synovium (p<0.01).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Serum concentrations of VEGF analysed and presented as described in the legend to fig 2.
Correlations between serum levels of soluble adhesion molecules and/or vascular endothelial growth factor and clinical findings
Table 3 shows the associations between clinical measures of disease activity and serum soluble adhesion molecules or VEGF concentrations in all patients with RA.
Correlations between serum concentrations of soluble adhesion molecules and/or vascular endothelial growth factor and clinical parameters in all patients with rheumatoid arthritis
About 67% and 75% of patients with RA, with diffuse and follicular synovitis respectively, were seropositive (table 1). No correlations between the patient's age, disease duration, or rheumatoid factor and any soluble adhesion molecules or VEGF levels were found. Although disease modifying antirheumatic drugs (DMARDs) were more often used among patients with the follicular histological form of the RA, the difference was significant only for methotrexate (p<0.05) (table 1).
DISCUSSION
Several studies emphasise the role of the endothelium in the pathogenesis of rheumatoid synovitis. The adhesion molecules, expressed on the endothelial cells, mediate the attachment of leucocytes and their extravasation out of circulation into rheumatoid synovium.17–20 The importance of CAMs in the pathogenesis of RA is confirmed by higher ICAM-1, VCAM-1, and E-selectin (endothelial leucocyte adhesion molecule-1 (ELAM-1)) expression in rheumatoid synovium even in the early stages of the disease, compared with the controls.19,20,27,28 The pathophysiological role of soluble forms of CAMs (sCAMs) is not completely understood. It was suggested that sCAMs might control the interactions between leucocytes and the cell surface forms of the molecules. Another possibility is that binding by sCAMs may regulate the activation of the leucocytes before they interact with the endothelium. Several reports suggest that raised levels of sCAMs may simply be an indicator of activation of endothelial cells.17–19,29,30
In our study the sICAM-1 concentration was significantly raised in all patients with RA. Furthermore, sICAM-1 reached the highest levels in patients with the follicular type of synovitis, distinguishing them from those with the diffuse pattern of synovitis. Numerous studies have shown high sICAM-1 levels in the serum of patients with RA,17,31–34 although, some reports showed that the rise in serum sICAM-1 in patients with RA was not significant.35,36 Previously we showed the presence of increased concentrations of sICAM-1 in patients with RA with vasculitis compared with patients with uncomplicated disease.31 Our findings were similar to those of other studies.17,35,36 Therefore, sICAM-1 may also be a useful marker of systemic vascular inflammation in patients with RA.
Several investigators have demonstrated significant associations between serum levels of sICAM-1 and ESR,31,35,37 CRP,38 rheumatoid factor,35 or joint count.37 The concentration of sICAM-1 in RA sera was also shown to correlate with sVCAM-117 or sE-selectin.17,32 However, others did not find associations between the serum levels of sICAM-1 and sVCAM-129 or between sICAM-1 and clinical markers of disease activity.29,34 We demonstrated correlations between serum sICAM-1 concentrations and sVCAM-1, sE-selectin, VEGF levels, ESR, CRP values, and number of swollen joints. Raised sICAM-1, especially in patients with RA with the follicular form of the disease, may be an indicator of endothelial cell activation, leading to migration of mononuclear cells into the rheumatoid synovium. Therefore, the serum concentration of this soluble adhesion molecule seems to be associated with a distinct histopathological manifestation of RA and reflects different clinical activity of the disease. Thus, follicular synovitis may be considered as a more active form of RA than diffuse synovitis.
Recently it was shown also that sVCAM-1 mediates mononuclear cell chemotaxis in RA.20 Furthermore, sVCAM-1 possesses angiogenic activity, which increases the delivery of mononuclear cells into the rheumatoid synovium.23 Several studies have demonstrated increased sVCAM-1 concentrations in RA serum.29,32,39 However, in another study, although sVCAM-1 was raised in RA serum compared with healthy subjects, the difference was not significant.33 Moreover, other investigators found that the sVCAM-1 level was lower in the serum of patients with RA than in controls.17 In our study we found that serum sVCAM-1 concentrations were higher in all patients with RA than in patients with OA. sVCAM-1 dominated in patients with follicular synovitis and could differentiate them from those with diffuse synovitis. Furthermore, we showed an association between sVCAM-1 and sICAM-1, VEGF, and with markers of disease activity such as ESR, CRP, and the number of swollen joints. Significant correlations were also noticed previously between serum levels of sVCAM-1 and ESR29 or CRP29,38 in patients with RA. Serum sVCAM-1 was also found by others to correlate with sICAM-1.17 However, in another study sVCAM-1 failed to correlate with the serum level of this soluble adhesion molecule.29 Some reports suggest that ICAM-1 and VCAM-1 may contribute to T lymphocyte activation and prevention of apoptosis of B and T cells.30 The highest serum concentrations of sICAM-1 and sVCAM-1 found by us in patients with the follicular type of synovitis may be responsible for B and T lymphocyte survival. Taken together all these finding suggest that RA is more active in patients with follicular synovitis.
It was shown also that sE-selectin mediates endothelial cell chemotaxis.23 Furthermore, sE-selectin expresses angiogenic activity, potentially increasing the ingress of mononuclear cells into inflamed RA synovial tissue.23,40 It is postulated that E-selectin, which is expressed very early in the rheumatoid process, may be important in triggering angiogenesis in the initial stages of RA.41 Our study demonstrated raised serum sE-selectin concentrations in all patients with RA and in patients with both histological types of the disease. Other reports have also shown increased sE-selectin levels in RA serum.17,36 In some studies the serum concentration of sE-selectin was increased in patients with RA relative to healthy controls, but those differences were not significant.32,33 We found associations between serum levels of sE-selectin and sICAM-1 and ESR as was found by other studies.17,32,42
VEGF is a potent mediator of endothelial proliferation, angiogenesis, and capillary hyperpermeability.21,43 Neovascularisation is one of the earliest observed features of RA within the synovium, which promotes the delivery of inflammatory cells.1,2,22 Therefore, it was suggested that VEGF might play a part in the pathogenesis of RA. Several studies have demonstrated higher VEGF concentrations in the serum of patients with RA than in controls.43–46 In our study, also, the serum levels of VEGF were significantly higher in all patients with RA than in those with OA. Furthermore, a higher VEGF concentration was found in patients with follicular synovitis than in those with the diffuse histopathological type of RA. Moreover, we showed that the serum concentration of VEGF correlated with serum levels of sICAM-1, sVCAM-1, CRP, ESR values, and the number of swollen joints. In other studies, also, VEGF in RA serum correlated with ESR,46 CRP,43,44,46 rheumatoid factor concentration, and the number of tender and swollen joints.46 Our results suggest that, as for serum sICAM-1 and sVCAM-1 concentrations, the VEGF serum level also is related to RA activity and associated with histological manifestation of the disease. Therefore, the serum concentrations of these molecules may be used as markers for identifying different histological forms of rheumatoid synovitis.
DMARDs may decrease the expression of sCAMs19 and VEGF.44 One possible explanation is that secretion of the proinflammatory cytokines responsible for adhesion molecule up regulation is reduced.20,32,34,40 Although DMARDs were more often used by patients with the follicular histological form of the RA, the difference was significant only for methotrexate. Moreover, the concentrations of sCAMs and VEGF were particularly raised among patients with follicular synovitis. Therefore, more aggressive treatment in those patients seems simply to reflect greater activity of the disease. Also radiological analysis demonstrated that more advanced joint destruction (stage III or IV according to Steinbrocker's criteria) was more common among patients with follicular synovitis. Others also have found an association between serum sICAM-1 concentrations and the radiological stages of the disease progression.35
There was no correlation between the soluble adhesion molecules levels and the leucocyte count (data not shown). This indicates that increased sCAM concentrations do not simply reflect a raised leucocyte population. We found no association between the sex, age, and disease duration of patients and the serum concentrations of sICAM-1, sVCAM-1, sE-selectin, or VEGF (data not shown); a similar lack of correlation was found by others.17,32
In our study we demonstrated significantly raised levels of sICAM-1, sVCAM-1, and VEGF in RA serum compared with patients with OA. Concentrations of these molecules were particularly raised in patients with the follicular form of synovitis, clearly distinguishing them from those with the diffuse type of the disease. This report shows that there are distinct profiles of the raised soluble adhesion molecules and VEGF in different histological forms of RA. Moreover, sICAM-1, sVCAM-1, and VEGF were found to correlate with laboratory and clinical markers of disease activity. All these data suggest that the activity of the disease is greater in patients with RA with follicular synovitis than in those with diffuse synovitis. Therefore, these molecules are not only good markers of disease activity but might also be used to determine the histopathological manifestation of RA. Our findings confirm the heterogeneity of RA and suggest the possibility of different responses to disease treatment. We conclude that the heterogeneity of RA should be considered when treatments are designed.
Acknowledgments
We thank our colleagues in the Department of Orthopaedic Surgery for providing synovial samples.