Article Text

Abstract
Aims—To see whether a correlation exists between clinicopathological parameters, argyrophilic nucleolar organiser regions (AgNORs), and nucleolar counts in the nuclei of tumour cells in patients with transitional cell bladder carcinoma.
Methods—Paraffin wax embedded sections from a total of 62 cases of primary transitional cell bladder carcinoma were stained with the silver colloid method. The numbers of individual silver grains (AgNORs) in nucleoli and the numbers of nucleoli were counted in 100 nuclei. The correlation between AgNORs and nucleolar counts and patients' sex, tumour grade, disease stage, recurrence pattern, and tumour related survival was analysed.
Results—The numbers of nucleoli in tumour cells were higher in male patients (p < 0.032). AgNOR numbers correlated with tumour grade (p = 0.017) and recurrence (p = 0.046). In multivariate analysis, the variation coefficient of AgNOR scores was found to be the only independent predictor of the duration of tumour free period in patients with recurrent disease (p < 0.002). AgNOR scores and nucleolar counts were of no value in distinguishing superficial and invasive tumours or in predicting tumour related survival.
Conclusions—AgNOR scores in transitional cell bladder carcinoma reflect variations in tumour biological behaviour; however, the clinical value of this technique in patients with urinary bladder carcinoma is limited.
- bladder neoplasms
- nucleolar organiser regions
- nucleoli
- prognosis
Statistics from Altmetric.com
The natural course of transitional cell bladder cancer is highly variable. The clinical approach to treatment is based mainly on the tumour stage and grade.1,2 However, the data obtained from these parameters are insufficient to predict the biological behaviour of an individual tumour. Therefore, additional criteria have been proposed as potential instruments for more accurate grading.3 Argyrophilic nucleolar organiser regions (AgNORs) are segments of DNA that are sites of ribosomal RNA transcription. Counting silver stained interphase AgNORs provides an estimate of cellular proliferation, and has been found to correlate with tumour grade and stage, and to bear independent predictive value in patients with urinary bladder carcinoma.4 However, the data obtained are controversial.5–7
The aim of our study was to estimate how the AgNOR and nucleolar counts in the tumour cells of transitional cell bladder carcinoma correlate with patients' sex, tumour grade, disease stage, recurrence pattern, and tumour related survival.
Materials and methods
Our study comprised 62 patients (48 men and 14 women), mean age 63.9 years (range, 32–88), with primary transitional cell bladder carcinoma who had been operated upon in the urological department, State Pavlov Medical University between 1985 and 1990. Patients were included if their specimens contained sufficient tumour material for AgNOR staining and if they could be followed for at least five years. Patients with invasive neoplasia were treated by radical and partial cystectomy. In cases with superficial tumours, transurethral resection was performed.
Follow up examination of patients with preserved bladder included cystoscopy every three months during the first year after surgery, cystoscopy every six months for the next two years, and then ultrasound sonography of the bladder followed by cystoscopy in suspect cases every one to two years. Thirty eight patients survived five years. Thirty seven patients developed recurrences, the mean (SD) recurrence rate being 24.8 (24.1) months (range, 2–90).
TISSUE
The tumour samples were fixed in 10% buffered formalin and embedded in paraffin wax. Sections (5 μm thick) were stained with haematoxylin and eosin. The tumours were graded as recommended by Mostofi and colleagues8 and staged postoperatively according to the TNM staging system.9 In 17 cases, specimens were too small to confirm the tumour stage.
AgNOR STAINING AND COUNTING
Sections (5 μm thick) cut in series with the haematoxylin and eosin stained sections were fixed in methanol/acetic glacial acid mixture (3/1) for 15 minutes and rinsed thoroughly with distilled water. After air drying, the sections were transferred to 2% formic acid and incubated for 10 minutes, rinsed again, and impregnated with silver nitrate solution, according to Howell and Black,10 with a slight modification, namely: two drops of gelatin solution were placed on the slide and mixed with four drops of freshly prepared 50% aqueous AgNO3 solution. The slides were covered by cover glasses, placed on to filter paper in a wet chamber (Petri dish), and incubated at 36°C for 18–20 minutes. The cover glasses were washed with distilled water. Then the slides were lightly counterstained in 2% Giemsa/phosphate buffer solution (pH = 6.8) for 10 seconds, rinsed three times in distilled water, air dried, and mounted. The numbers of individual silver grains (AgNORs) in nucleoli and the numbers of nucleoli in 100 nuclei were counted under oil immersion at a magnification of ×1000, after sharp focusing of the fine granular nuclear matrix.
STATISTICAL ANALYSIS
The mean numbers, maximum numbers, and variation coefficients (CV) of AgNORs and nucleoli of all nuclei for each section were calculated and expressed as the mean (SD). The student's t test, ANOVA/ANCOVA, log rank analysis, and multiple regression coefficients were applied.
Results
AgNOR and nucleolar scores were of no value in predicting death from transitional cell carcinoma. There was a significant increase in the mean AgNOR counts from grade I to grade II (t = 2.418; p < 0.020) and grade III (t = 2.334; p < 0.023). AgNOR counts overlapped (table 1), mainly between grades II and III. The strong correlation between AgNOR mean values and tumour grade was confirmed by ANOVA/ANCOVA (F = 4.325; p = 0.017), whereas the distribution of nucleoli was not dependent upon the grade. Neither mean AgNOR count nor nucleoli numbers could be used to distinguish between patients with superficial or invasive tumours because of considerable overlap (table 2). However, a significant difference between pT2 and pT3 tumours was found for both parameters (t = 3.490; p = 0.003 and t = 2.169; p = 0.047, respectively) as well as for mean AgNOR scores between pTa and pT3 (t = 4.558; p = 0.001).
Mean numbers of AgNOR scores and numbers of nucleoli as related to histological grade
Distribution of AgNOR scores and numbers of nucleoli as related to pathological stage
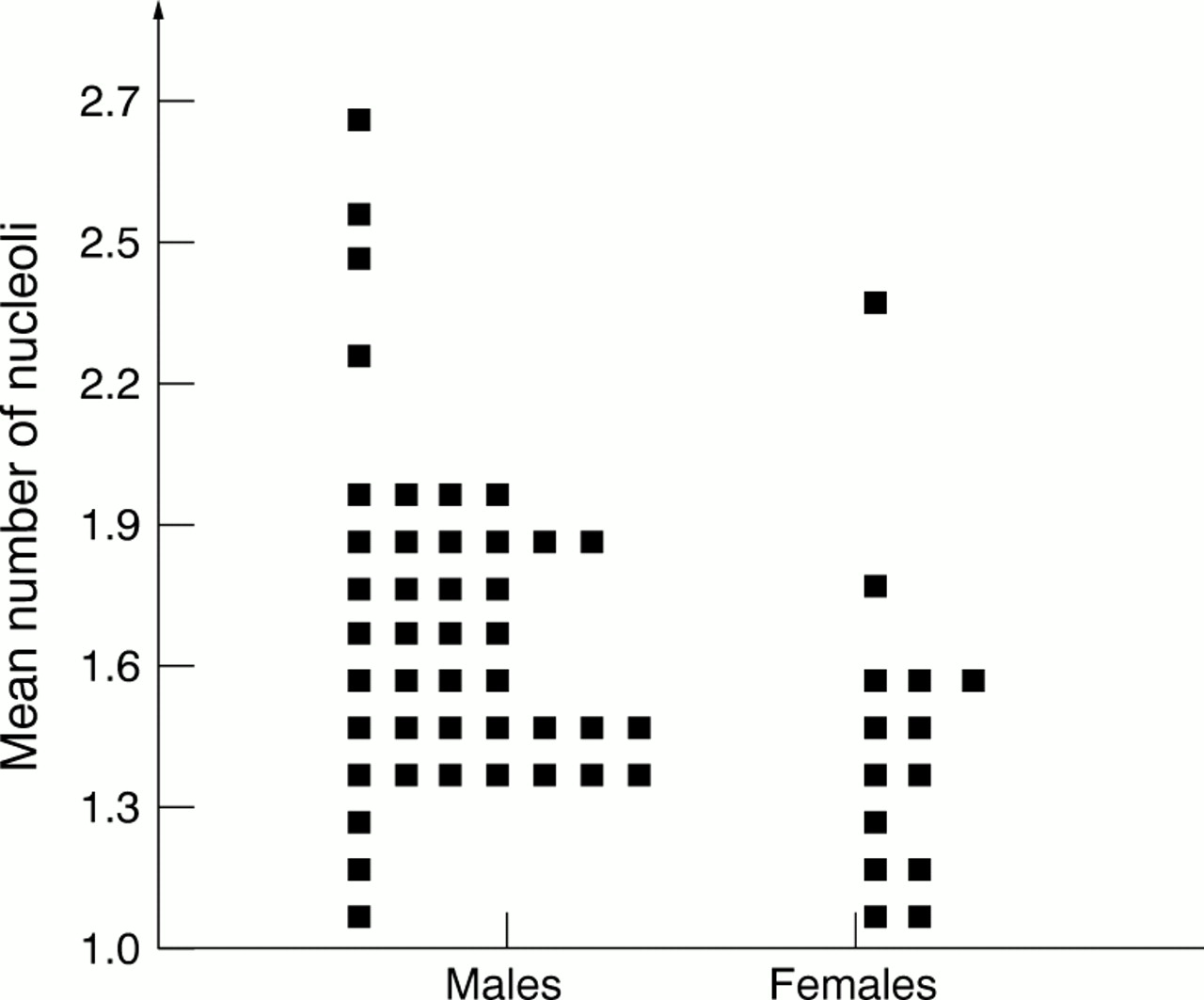
The mean AgNOR counts were not related to patients' sex (table 3); however, the numbers of nucleoli in tumour cells were higher (t = 2.108; p = 0.039) in male patients (fig 1). The significance of the male to female difference of nucleolar distribution was also supported by multiple regression analysis (R2 = 0.65; F = 4.87; p < 0.032).
Mean numbers of AgNOR scores and nucleoli as related to patients' sex
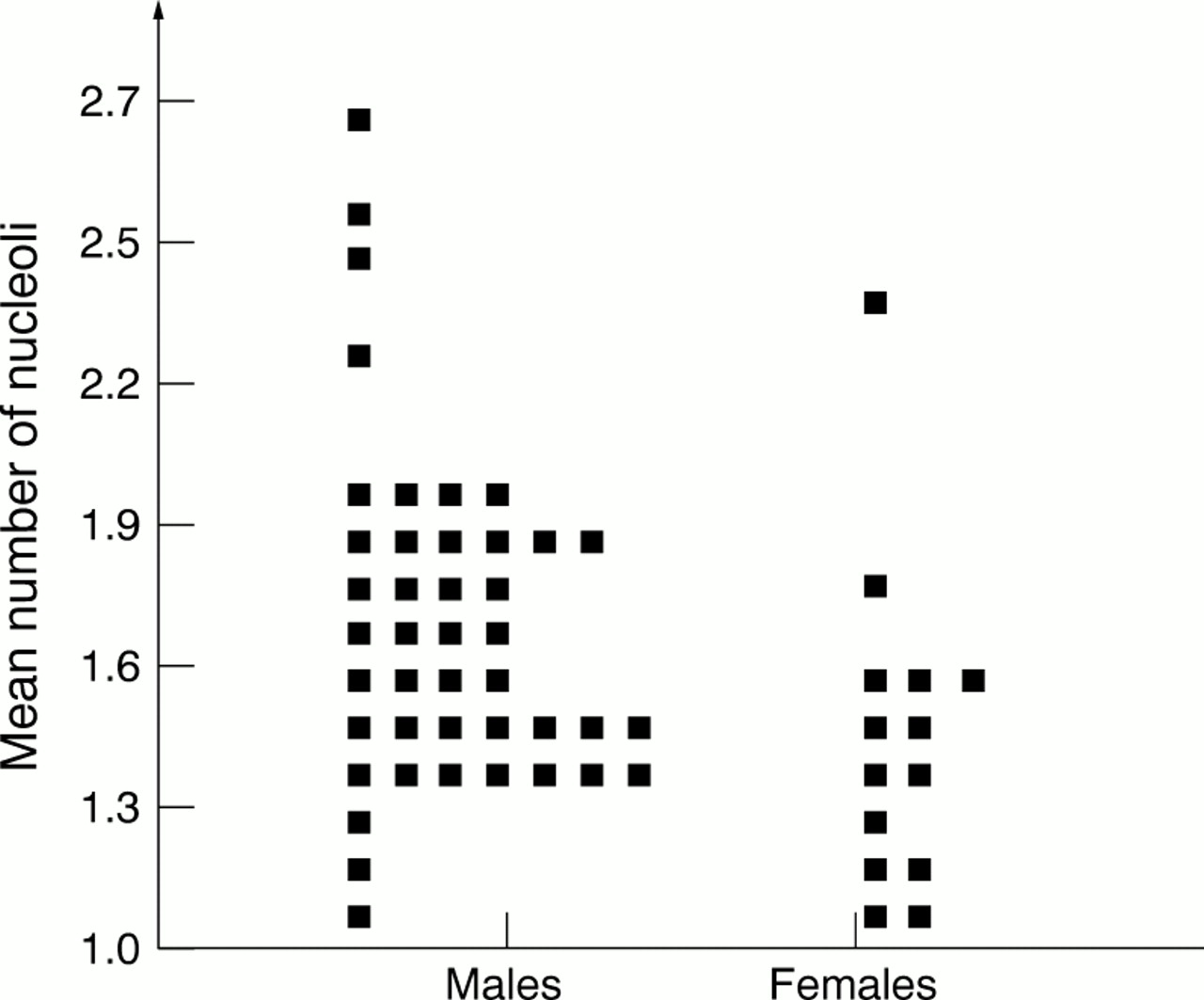
Mean numbers of nucleoli in tumour cells in male and female patients with bladder carcinoma.
The mean and maximum values of AgNOR counts and numbers of nucleoli showed overlap in patients with and without recurrences (table 4). However, patients with recurrences harboured the tumours with higher AgNOR and nucleolar scores. Significant differences were found between maximum AgNOR scores (t = 2.039; p = 0.046) (fig 2A) and nucleolar scores (t = 2.530; p = 0.014) (fig 2B).
Mean and maximum values of AgNOR scores and numbers of nucleoli as related to recurrence pattern
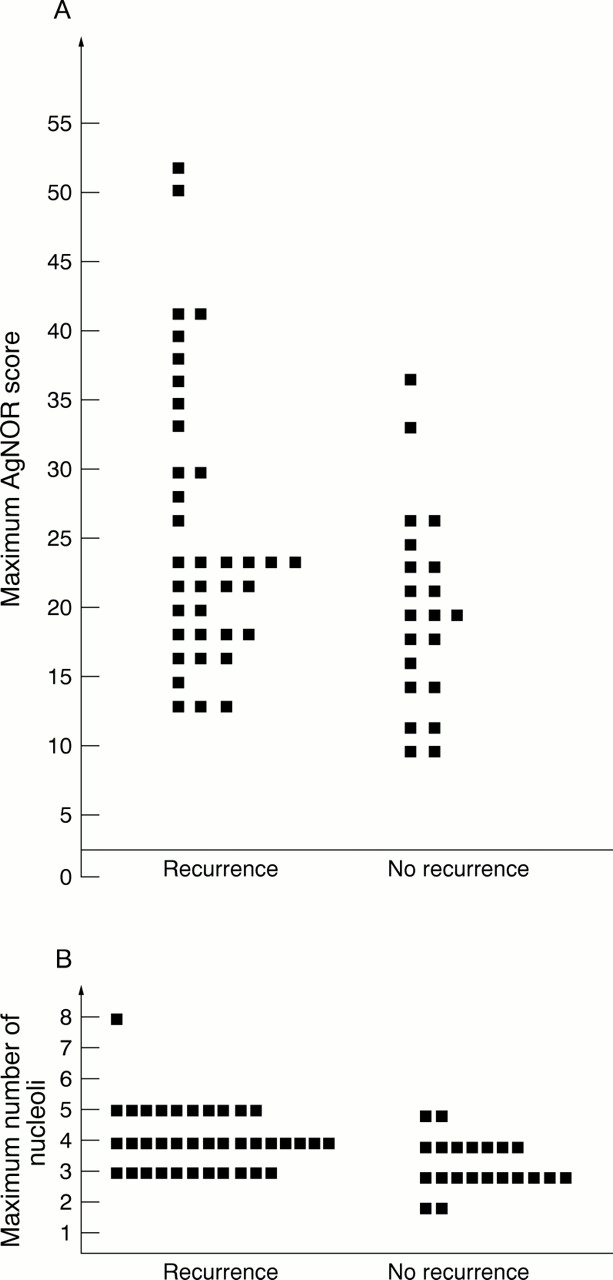
(A) Maximum numbers of argyrophilic nucleolar organiser regions (AgNORs) in tumour cells of patients with recurrent and non-recurrent bladder carcinoma. (B) Maximum numbers of nucleoli in tumour cells of patients with recurrent and non-recurrent bladder carcinoma.
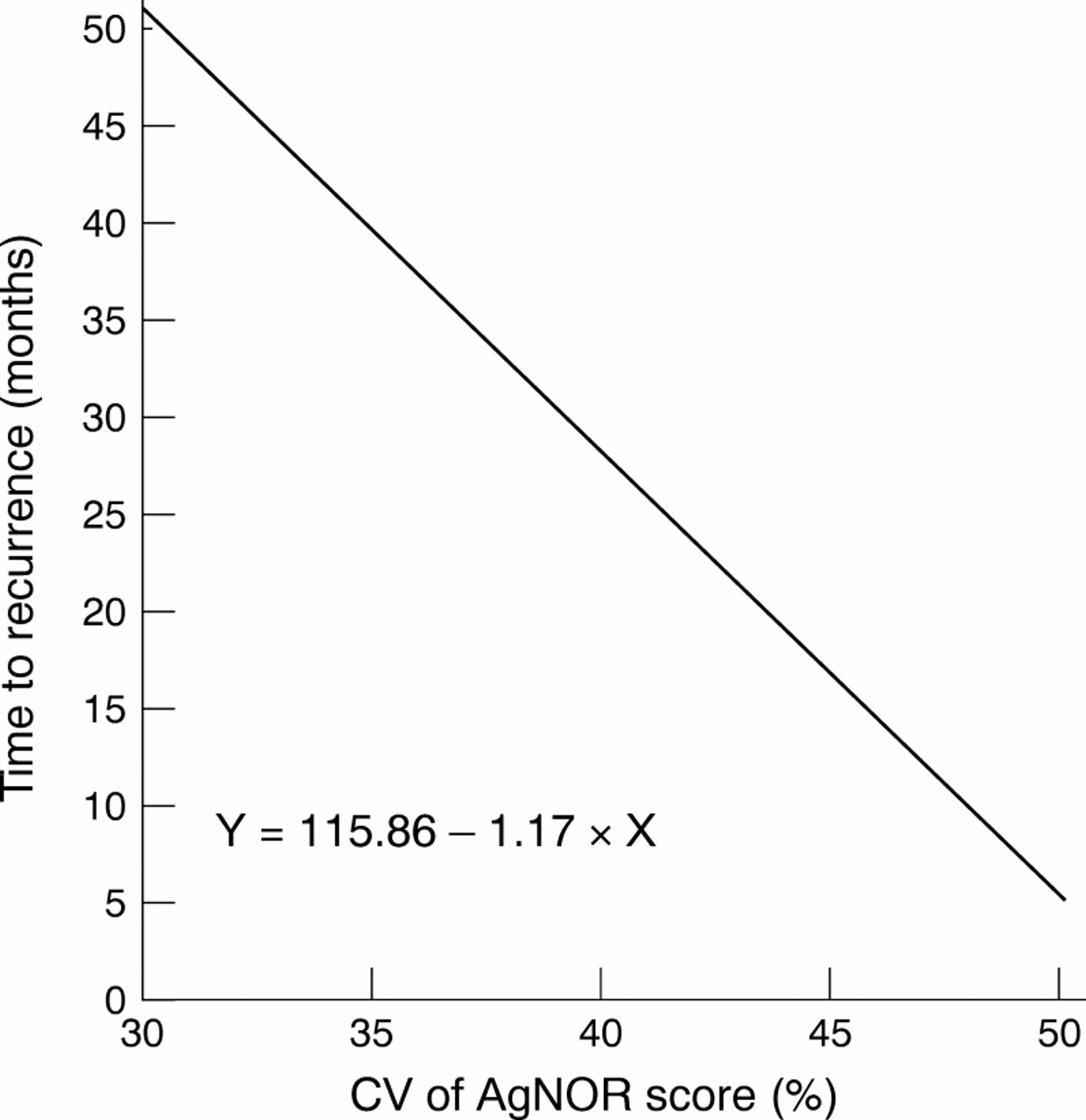
Of note, is that the CV of AgNOR scores in multiple regression analysis was strongly correlated with duration of the tumour free period in patients with recurrent disease (R2 = 0.24; F = 12.17; p < 0.002) (fig 3).
{kind=link}
{kind=link}
{kind=link}
Correlation between variation coefficient (CV) of argyrophilic nucleolar organiser region (AgNOR) score and duration of tumour free period in patients with recurrent urinary bladder carcinoma.
Discussion
AgNORs are segments of DNA that transcribe ribosomal RNA. The numbers of these regions in each nucleus correlate with cellular activity and, therefore, may serve as an indicator of the degree of malignant potential in tumours.11,12 In our study, we found that higher grade tumours tended to have higher AgNOR scores than their low grade counterparts, presumably because of the higher proliferation status of less differentiated carcinomas. The difference between grades I–II and I–III was evident; however, it was not found between grades II and III. The latter observation might reflect a slight difference in proliferation states between grades II and III, and to some extent might be explained by the subjectiveness of grading as a qualitative method, with considerable intraobserver and interobserver variations.
The AgNOR scores and numbers of nucleoli showed a trend to increase with tumour pathological stage; however, significant differences in the counts were noticed only between deeply invasive (pT3) and more superficial neoplasms. This finding might be explained by the close relation between histological grade and pathological stage (p < 0.001). Therefore the association of AgNORs with tumour stage was mainly secondary to their relation to tumour grade. Of note, was a reduction in AgNOR and nucleolar counts in T4 tumours which, although not significant, could indicate a decrease of proliferation state of highly extensive neoplasms.
The dissimilarity between nucleolar distribution seen in male and female patients is not completely understood. It is known that bladder cancer is nearly three times more common among men than women, a fact that might be explained by differences in genetic mechanisms,13 hormonal status,14 or an anatomical predisposition to urinary retention and exposure to industrial and environmental carcinogens in men. Our findings suggest that there is a higher proliferation potential of bladder neoplasms in men. We have also observed a lower rate of tumour related survival in men than in women (log rank analysis: p = 0.005), presumably associated with higher cellular activity in men, which can be measured, to a certain extent, by nucleolar silver staining.
AgNOR counts and numbers of nucleoli were highest in tumours from patients with recurrent disease, therefore supporting their high malignant potential. However, in multiple regression analysis mean and maximal AgNOR scores, histological grade, and pathological stage did not predict the duration of the disease free period. The sole predictor found was the CV of the AgNOR score, demonstrating that in our study a recurrent course of urinary bladder carcinoma was predominantly related to high heterogeneity of cell proliferation states. It has been shown recently that proliferating cell AgNORs have a predictive value for local recurrence in patients with superficial bladder tumours.15
In conclusion, we have shown that AgNOR counts in transitional cell urinary bladder carcinomas are closely related to the histological grade and indirectly to the depth of tumour invasion, but not to tumour related survival. We also found a correlation between nucleolar distribution and the patient's sex, indicating potential differences in proliferative activity between urinary bladder carcinoma in men and women. We found that interphase AgNOR counts cannot be used to distinguish patients with and without a recurrent course of disease. However, the CV of the AgNOR score was found to be the best predictor of the duration of recurrence free period. These findings suggest that AgNOR scores give additional cell kinetic information in patients with urinary bladder carcinoma and reflect variations in tumour biological behaviour. However, the clinical value of this technique is limited.