Article Text

Abstract
Background/Aims:Helicobacter pylori gastritis is a risk factor for the development of gastric cancer. The results of several studies indicate that gastric adenomas, which are considered premalignant lesions, may also be associated with H pylori gastritis. However, it is not clear whether there are different patterns of gastritis in these patients compared with patients with gastric cancer or patients with H pylori gastritis alone. Therefore, this study was designed to investigate the patterns of gastritis in these three groups of patients.
Methods: The histological features of gastric mucosa at a distance from the tumour were analysed prospectively in 118 patients with gastric adenoma (mean age, 71.8; female to male ratio, 6 : 4). In addition, for every patient with H pylori associated gastric adenoma an age and sex matched control patient with either H pylori associated early gastric cancer of the intestinal type or H pylori gastritis only was investigated.
Results: Only 60 patients (50.9%) with gastric adenoma were infected with H pylori. In the remaining patients, complete atrophic gastritis predominated. In those patients with adenoma and H pylori infection, the gastritis was similar to that seen in patients with early gastric cancer (median score, 2 for activity and degree of gastritis in the antrum and corpus); intestinal metaplasia was common to both groups. These two groups differed significantly from patients with H pylori gastritis only (median grade and activity of gastritis, 1 in antrum and corpus), in whom intestinal metaplasia was rare.
Conclusions: It appears that gastric adenomas and gastric intestinal cancer arise by analogous mechanisms. However, owing to severe atrophic gastritis and a lower incidence of H pylori, adenomas do not appear to be definite precursor lesions for gastric cancer.
- Helicobacter pylori
- gastritis
- gastric cancer
- gastric adenoma
Statistics from Altmetric.com
It is known that infection with Helicobacter pylori always causes chronic active gastritis. Infection with the bacterium provokes invasion of the mucosa by lymphocytes/plasma cells (a marker for the grade of gastritis), and neutrophils (a marker for the activity of gastritis). In addition to these diffuse parameters, multifocal features such as intestinal metaplasia, atrophy, and lymphoid follicles may also be found in association with H pylori infection.1
For gastric cancer of the intestinal type, Correa suggested a human model of carcinogenesis. He postulated that hyperproliferation caused by H pylori gastritis is the starting point of a sequence leading to gastric cancer.2 This hyperproliferation may then initiate DNA alterations. The mutation of several antigens, such as Lewis a and carcinoembryonic antigen, suppressor genes, such as p53, or oncogenes, such as c-myc, APC/β catenin, or ras, might be associated with the evolution from normal gastric mucosa to carcinoma.2,3 These changes are represented histopathologically by superficial gastritis leading to multifocal atrophy, intestinal metaplasia and, finally, dysplasia/cancer.2 It has also been reported that cancers may develop via gastric adenomas4; hence—as for the carcinogenesis of colorectal carcinomas5—adenomas have been regarded as premalignant lesions.4
“Infection with Helicobacter pylori always causes chronic active gastritis”
However, data on gastric adenomas are still very sparse and, surprisingly, the incidence of gastric adenoma is much lower than that of gastric carcinoma.6,7 Hence, most gastric cancers do not develop via adenomas. In addition, in contrast to gastric cancer, little is known about the features of gastritis associated with gastric adenomas. This background prompted us to conduct a study, first to investigate the histopathological features of gastric adenomas—in particular the surrounding mucosa—and then to compare these findings with the patterns of gastritis in patients with early gastric cancer of the intestinal type and patients with gastritis alone.
PATIENTS AND METHODS
We analysed retrospectively all gastric adenomas investigated histopathologically at the pathological institute of Bayreuth between 1969 and 1996. For inclusion in the study, additional biopsies from the antrum and corpus mucosa at a distance from the tumour also had to be available; a total of 118 patients met these criteria. At the time of diagnosis, the patients’ mean age was 71.8 years (SD, 11.37; range, 34–93). Forty seven patients (39.8%) were men and 71 (60.2%) were women. With the exception of one patient with an adenoma of the pyloric gland type (0.8%), all adenomas were of the intestinal type. Figure 1 shows the location of the adenomas in the stomach.
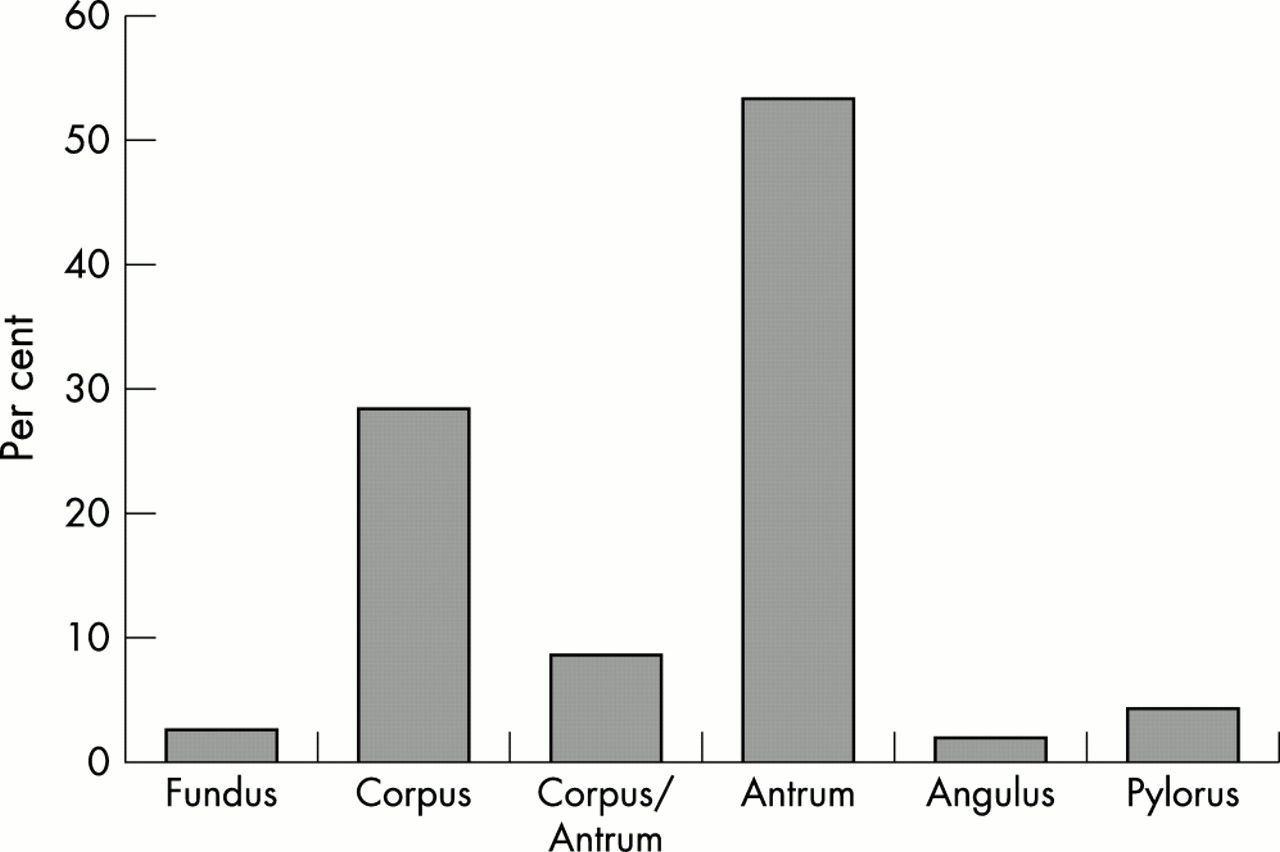
Location of gastric adenomas (n = 118).
In addition, we included 60 patients with early gastric cancer of the intestinal type and histological evidence of H pylori, and a further 60 patients with H pylori gastritis not associated with peptic ulcer or gastric malignancy. These patients had been matched by age (± 2 years) and sex to the 60 H pylori infected patients with gastric adenoma. Data from the patients with H pylori associated gastric cancer and from those with H pylori gastritis alone were also collected retrospectively from the histopathological record forms at the pathological institute of Bayreuth. For patients with gastric adenoma, two biopsies from the antrum and corpus (patients with early gastric cancer, at least 5 cm distant from the tumour) were also required. Matching was effected blind to the results of the histopathological examinations with the exception of H pylori status.
Paraffin wax embedded samples were sectioned and stained with haematoxylin and eosin and the Warthin-Starry stain for the detection of H pylori. All histological data were evaluated by a single experienced pathologist (MS). Gastritis was evaluated in accordance with the updated Sydney system,1 with the exception of intestinal metaplasia in the antrum or corpus, which was simply noted as present or absent, but not further subclassified.
For statistical analysis, analysis of variance (ANOVA) was used to compare age in the three groups. Features of gastritis (degree and activity of gastritis, presence of intestinal metaplasia) were compared using the χ2 test or Fisher’s exact test. A p value of less than 0.05 was considered significant.
RESULTS
Of the 118 patients with gastric adenoma, 60 patients (50.9%) were infected with H pylori. In the remaining 58 patients, autoimmune gastritis in the corpus was the predominant pattern, characterised by complete atrophic gastritis in 48 patients (40.7%) and partial atrophy with active destruction of the corpus glands and hyperplasia of parietal cells in two patients (1.7%). Eight patients (6.8%) had gastritis with typical features of an earlier H pylori infection; that is, the presence of lymphoid aggregates, moderate lymphocytic infiltrate, but no detectable organisms (fig 2).
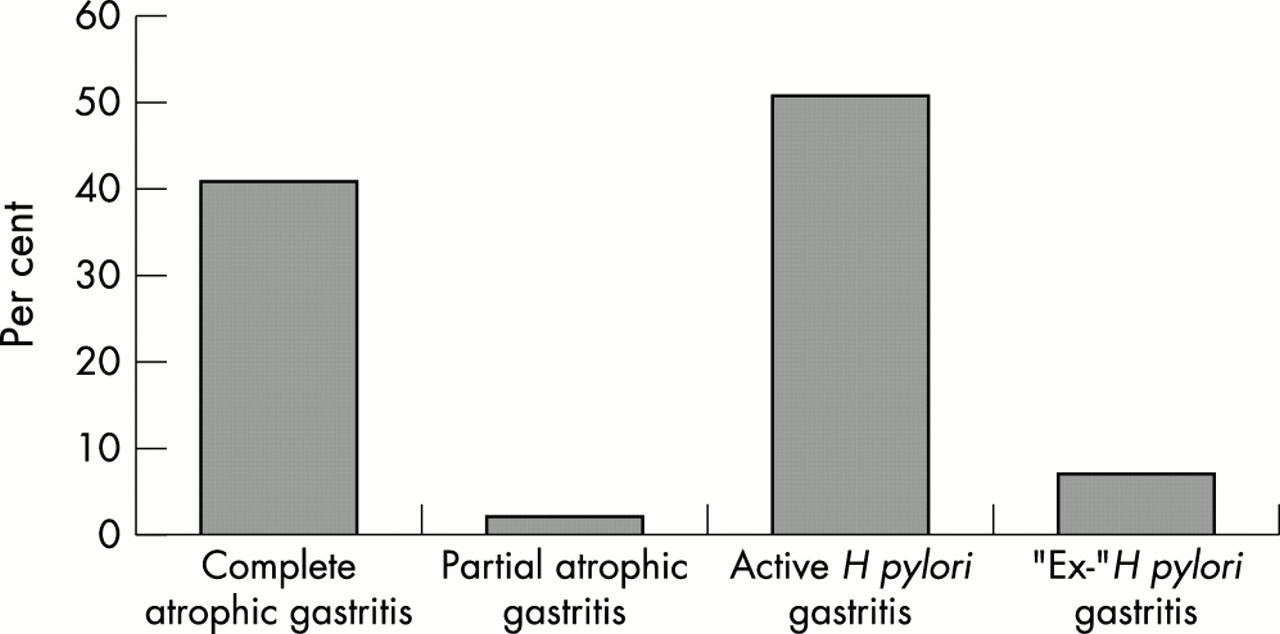
Classification of gastritis in patients with gastric adenomas (%) (n = 118).

{kind=link}
{kind=link}
{kind=link}
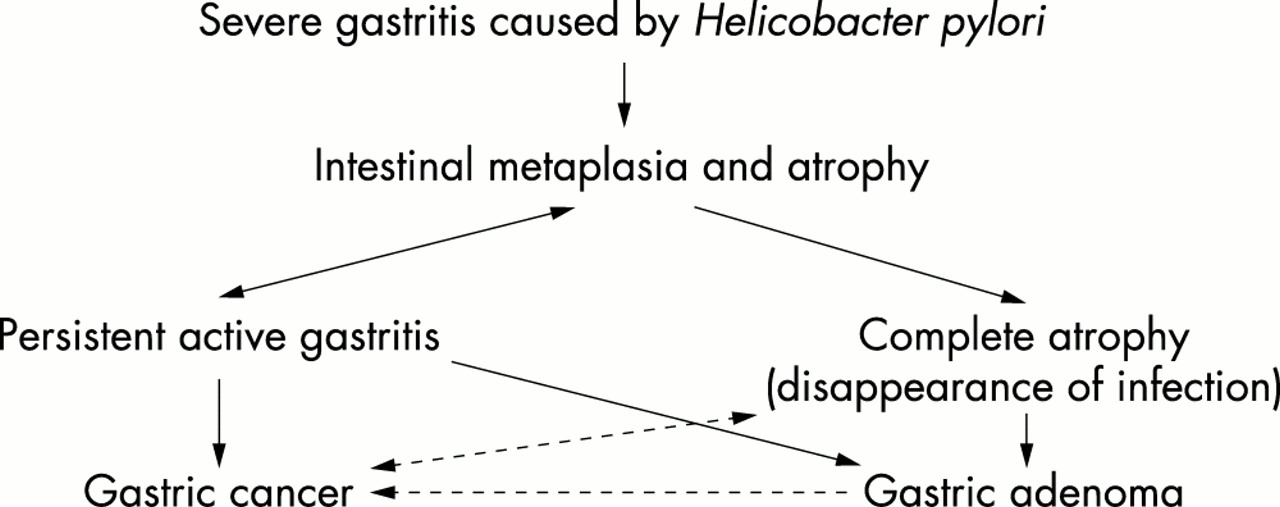
Possible pathways leading from Helicobacter pylori gastritis to either gastric adenoma or gastric cancer.
No differences were seen between the mean ages of the three matched groups with H pylori infection and either gastric adenoma, early gastric cancer, or H pylori gastritis alone (adenoma, 69.5 years; cancer, 68.6 years; gastritis, 69.6 years; all p > 0.5). However, there were highly significant differences in terms of the grade and activity of H pylori gastritis in the antrum or corpus in patients with H pylori gastritis alone in comparison with the other two groups. In these last two groups, gastritis in the antrum and corpus was more severe than in patients with gastritis alone (median grade and activity 2 v 1; tables 1 and 2). In addition, intestinal metaplasia in the antrum or corpus was more frequently present in the two groups with gastric tumours than in the group with gastritis only. The presence of intestinal metaplasia in the antrum was most prominent in the group with gastric cancer, whereas in the corpus this feature was more often present in patients with gastric adenoma. However, these differences between the two groups were not significant (tables 1 and 2).
Differences in Helicobacter pylori gastritis in the antrum
Differences in Helicobacter pylori gastritis in the corpus
DISCUSSION
Our data show that the proportion of patients with gastric adenoma and H pylori infection is lower than that reported for patients with early gastric cancer. Only 50.9% of the patients with gastric adenoma were infected with the organisms, whereas our own previously published data, in addition to data from others, show incidence rates of H pylori infection of around 80–90% for those with early gastric cancer.8–11 However, when H pylori was detected, gastritis parameters were similar in patients with gastric adenoma and early gastric intestinal cancer. In both groups, H pylori gastritis was comparatively severe in the antrum and the corpus, and intestinal metaplasia was a common finding.
In light of the fact that both H pylori infection and gastric adenomas are thought to be premalignant lesions in a sequence leading to gastric cancer, why was H pylori infection in the group of patients with gastric adenoma less frequent than expected? If there really is a sequence of H pylori gastritis → metaplastic changes → adenoma → carcinoma, one would expect to find at least as many H pylori infected patients with a “premalignant” adenoma as with gastric cancer.
However, in those patients with gastric adenoma but no concomitant H pylori, either body predominant atrophic gastritis (∼ 43%) or gastritis showing the typical features of an earlier H pylori infection (∼ 7%) was diagnosed. These data are in agreement with other reports showing a similarly high frequency of complete atrophy in the adenoma bearing stomach.12,13 Therefore, the incidence of complete atrophic gastritis in patients with gastric adenoma is much higher than in the general population14 or in populations with confirmed gastric cancer.8 We now know that in some cases infection with H pylori can induce severe inflammation with destruction of the corpus glands (“pre-atrophic stage”), which finally leads to complete atrophy of the corpus mucosa (“atrophic stage”).15,16 This stage of atrophy with loss of acid production does not favour the growth of H pylori.17 Thus, in some cases, H pylori may no longer be detectable, even though it initially induced the mucosal damage. Hence, we speculate that the high incidence of atrophic gastritis in the group of patients with gastric adenoma might reflect a “burned out” mucosa as a response to long lasting severe H pylori gastritis. In addition, the remaining 7% of patients with neither H pylori nor atrophic gastritis showed the typical features of gastritis often found after eradication of the organism.18,19
However, when H pylori was present the gastritis resembled the gastric cancer phenotype of H pylori gastritis (that is, severe gastritis in the antrum and corpus, high percentage of intestinal metaplasia).20,21 Therefore, it could be speculated that this pattern of gastritis initially induced by H pylori causes both gastric adenoma and gastric cancer. However, the observation that many more patients develop cancer rather than adenoma,6,7 and that a comparatively high proportion of patients with gastric adenoma develop complete atrophy, whereas most patients with early gastric cancer still have active H pylori gastritis, remains to be clarified. A possible explanation could be that adenomas are relatively slow growing neoplasms so that the surrounding mucosa more often reaches an “end stage” of atrophic gastritis. In contrast, cancers progress more rapidly and fewer patients will reach complete atrophic gastritis before detection.
“The high incidence of atrophic gastritis in the group of patients with gastric adenoma might reflect a `burned out’ mucosa as a response to long lasting severe H pylori gastritis”
Of interest in this regard are data published by Hattori from Japan.22 On analysing gastric microcarcinomas of the intestinal type (diameters < 5 mm) he found no precursor lesions in the tumour margins, and concluded that intestinal metaplasia, dysplasia, and carcinoma arise coincidentally. This implies that no precursor is present for either of them, which is in direct contradiction to the Correa model postulating a cascade ending in gastric cancer. On the basis of Hattori’s data, it might be speculated that severe gastritis caused by H pylori infection leads to a constant cellular stress. As a result, the following mechanisms may be triggered: the cells of the mucosa undergo apoptosis leading to atrophy, or they become metaplastic (intestinal metaplasia), or—in the worst case—dysplastic. Hence, in contrast to colorectal cancer, we do not believe that there is a sequence of events beginning with gastritis leading to gastric adenoma and finally ending in gastric cancer of the intestinal type. In our opinion, mucosal stress is reflected by epithelial alterations such as metaplasia and/or atrophy, which may therefore be regarded as markers for an increased risk of gastric cancer. This does not mean that malignant growth derives from metaplasia/atrophy, making the latter a condition for the development of the former. The reason why far more cancers develop in active severe H pylori gastritis and not in complete atrophic gastritis, which, in contrast, is found disproportionately more often in association with gastric adenomas, might be the fact that active inflammation leads to a series of changes that are probably involved in carcinogenesis: the ammonia produced by H pylori,23 increased cell proliferation,24,25 increased production of free oxygen radicals,26 and the increased production of nitric oxide27 may all trigger mutations in the stem cells. The development of intestinal metaplasia and/or atrophy might therefore be a physiological reaction of the gastric mucosa aimed at protecting itself from the constant stress caused by H pylori. If this theory were correct, one would expect adenomas with active H pylori associated gastritis in the surrounding mucosa to show an average higher grade of dysplasia. However, in our study only low grade dysplasia was found in adenomas, perhaps because most of the adenomas under investigation were not removed in total to check for areas with high grade dysplasia. It would be interesting to investigate whether adenomas with higher grades of dysplasia are indeed associated to a greater extent with active gastritis, similar to that found in early gastric cancers.
Take home messages
-
Both gastric adenoma and gastric cancer of the intestinal type appear to arise in severely inflamed mucosa caused by Helicobacter pylori infection
-
In contrast to early gastric cancers, gastric adenomas are more often found in association with complete atrophic gastritis in the body and are not necessarily premalignant lesions that will definitely lead to gastric cancer
-
The different pathways that lead to either benign or malignant tumour growth need to be investigated further