Article Text

Abstract
Aims: To improve the interpretation of immunohistochemistry (IHC) staining results the use of a tissue microarray technique was established in a routine setting.
Methods: A tissue microarray was constructed by harvesting 600 μm tissue cores from paraffin wax embedded samples available in a routine pathology department. The punches originating from non-tumorous tissue were placed on host paraffin wax blocks. The microarray contained 12 different tissue samples, with a wide antigen profile and a dimension of 3.5 × 3 mm. One section of the multitissue array was placed as an “internal” positive control on each slide of the patient tissue to undergo identical immunohistochemical procedures.
Results: Using the tissue microarray technique as a tool for internal quality control, the interpretation of immunohistochemical staining of more than 20 different antigens in routine IHC was improved. The tissue microarray did not influence the staining results in conventional IHC or in different automated IHC settings.
Conclusion: The regular use of an institution adapted tissue microarray would be useful for internal positive control in IHC to enable different laboratory demands. Furthermore, this technique improves the evaluation of staining results in IHC.
- immunohistochemisty
- tissue microarray
- quality control
Statistics from Altmetric.com
Immunohistochemical methods are routinely used in surgical pathology. For confidence in the immunohistochemistry (IHC) result it is necessary to perform valid quality controls.1–5 An internal positive control in IHC is essential to ensure that the immunostaining is working properly. A separate slide containing tissue known to be immunoreactive with the test antibody (external control) is a widely used but costly method. Furthermore, it does not completely guarantee that IHC has worked properly for the patient tissue. In many institutes, different positive control tissues for each test case are already in use, but these are often associated with logistical difficulties. The use of multitissue blocks in IHC has been described previously.6 The tissue microarray technique was invented by Kononen et al in 19987 and is a promising tool in modern pathology, with almost an infinite number of applications.8 We established a tissue microarray, which serves as a positive control microarray, as a new application for the tissue microarray technique. Because of the small size (3.5 × 3 mm) of the microarray, the staining of the test tissue was not affected and there was a clear demarkation of control and test tissue.
METHOD
We took core needle biopsies with a diameter of 0.6 mm from donor paraffin wax embedded tissue blocks of 12 different tissues (table 1), obtained from our routine histological workload, using a dedicated tissue array instrument (Beecher Instruments, New Jersey, USA). These tissue cores were arrayed into “host” paraffin wax blocks of 15 × 15 mm, creating similar arrays of 4 × 3 dots (fig 1) in the different blocks. To combine donor cores with the recipient block, the paraffin wax was reheated for five minutes at 80°C. At least 110 to 150 sections of 5 μm were cut and mounted on to adhesive coated slides and stored in a dry environment until use. A paraffin wax sectioning aid system (as described previously) was not used.7 Two different automated staining systems from Dako (Autostainer and TechMate; Glostrup, Denmark) were used for immunohistochemical staining, in addition to manual procedures. Table 1 lists the antibodies used for staining.
Control tissues used for immunohistochemistry
{kind=link}
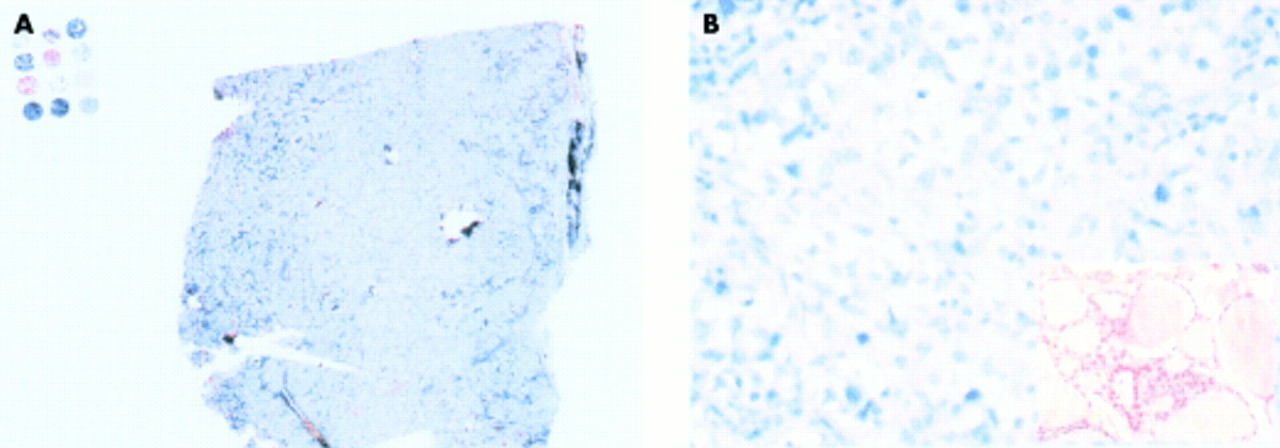
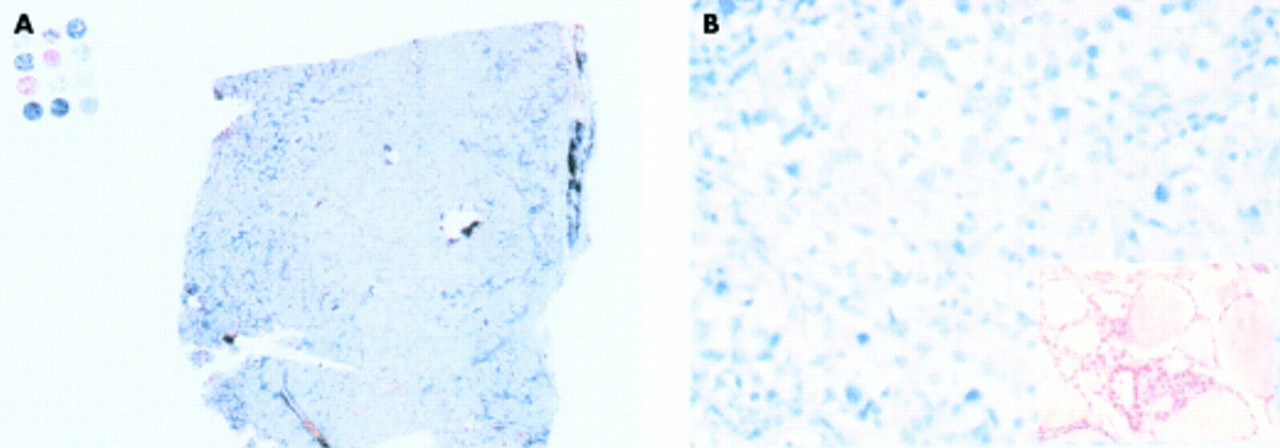
(A) Multitissue control array mounted at the end of the slide near to a tumour sample. (B) Magnification of the tumour stained negative for thyroid transcription factor 1 (TTF-1) with a missing staining reaction of the internal positive control. The positive staining result of the thyroid array element showed that the immunostaining had worked properly (inset right corner).
RESULTS
The microarray positive control tissue array blocks were used over a period of six months for 1000 test cases. There was an overall loss of control dots of < 1.5% while processing. A loss of staining after storage of multitissue sections (up to three to four weeks) was not seen. In general, the positive control dots stained brightly (fig 1), and non-specific staining patterns could easily be excluded. Antibody and antigen retrieval problems resulted in the failure of staining in individual slides in about 1.4% of the test cases. In most of these cases, the control tissue also showed a negative staining reaction, which prompted a repetition of IHC. The time taken for the preparation of the control slides was low, even when it was divided into array building and cutting. It took about five minutes to construct the 12 dot array, and 20–30 minutes for the cutting and mounting of 150 control slides.
DISCUSSION
The use of an internal positive control is the most reassuring method for quality control in IHC, with multitissue controls being the most effective. Nevertheless, the preparation of multitissue blocks (so called “sausage technique”) is time consuming and complicated in a routine setting. However, the microarray technique described here for building multitissue controls was easier and less time consuming because the control tissues for the multitissue blocks could be harvested from pre-existing blocks of paraffin wax embedded tissue. The consumption of “donor” tissue was low—0.6 mm tissue cores were sufficient so that the availability of rare tissues, particularly tumours with overexpression of tumour specific markers (for example, c-erbB-2 in breast cancer), was better than for conventional techniques. In addition, the amount of time needed for the preparation of a microarray control block was lower than described previously.9,10 However, at the moment the costs for the array instrument cannot be neglected, but we solved this problem by a multi-institute cooperation. In the near future, the wider use of these arrays should lead to the commercial availability of costume designed test blocks, which would circumvent this limitation. Other equipment or special tools that are not available in a routine histopathology laboratory are not required. In addition, the amount of microarray control tissue on individual slides is low, so that the amount of case tissue samples needed is not affected. It is also worth mentioning that the volume of antibody required is not increased. The control array did not affect the staining of the case tissue and there was always a clear demarkation between control tissue and the patient sample.
“The amount of time needed for the preparation of a microarray control block was lower than described previously”
Because this control array can be modified it could easily be adjusted to meet the individual needs of different laboratories. It is possible that arrays with dots of 5 × 5 (25 different tissues) could be devised, enabling the determination of a very wide antigen spectrum. The space required would be only 4.5 × 4.5 mm. This technique could also be applied to other staining procedures, such as fluorescent staining methods and brightfield in situ hybridisation.11
Aging of the tissue on the pre-prepared slides did not seem to influence the IHC results. Any possible aging, with consecutive loss of the immunoreactivity, would result in a false negative staining pattern of the internal control tissue, which would lead to repeated testing for that particular antigen. The heterogeneity of the donor tissues with regard to the different antigens might be seen as a disadvantage of this technique. Nevertheless, because the core biopsies function as “positive internal controls”, negative staining of the tissue microarray for a specific antigen in a specific dot would lead to it being withdrawn from further use.
We found that the control microarray could also be used with different automated IHC staining systems, and could be useful for monitoring the efficiency of the staining procedure by comparing the immunohistochemical staining intensity in different batches.
In conclusion, the internal multitissue control in IHC is a new application for the tissue microarray technique. We suggest that quality control in IHC would benefit from the use of multitissue microarray controls.
Take home messages
-
The tissue microarray technique is a useful new approach to internal multitissue control in immunohistochemistry (ICH)
-
The quality control of IHC would benefit from the use of multitissue microarray controls
Acknowledgments
This research was supported by the following grant: Innovative Medizinische Forschung Münster BÜ 2 2 00 18.